Introduction
The advent of video laryngoscopy has revolutionized airway management in both pre-hospital and hospital settings, providing unparalleled visualization and improving intubation success rates【1】. However, the traditional Macintosh (Mac) blade, originally designed for direct laryngoscopy, poses unique challenges when paired with video technology. The hypercurved Mac blade, specifically engineered for video laryngoscopes, introduces a distinct approach that requires an understanding of its unique geometry and technique【2】.
This article aims to highlight the key differences between the hypercurved Mac blade and the traditional blade, providing clinicians with guidance on maximizing the utility of this advanced airway tool.
Understanding the Hypercurved Mac Blade
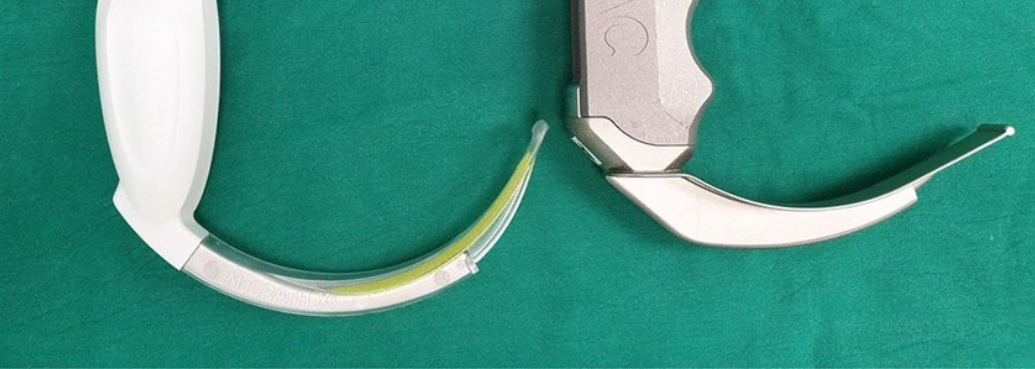
The hypercurved Mac blade, sometimes referred to as a “hyperangulated” or “hypercurved” blade, features a more pronounced curvature compared to its standard counterpart. This design optimizes the view of the glottis on the video screen by enhancing the angle of approach, making it easier to navigate around anatomical structures that may obstruct visualization during direct laryngoscopy【3】. However, this modification also changes the mechanics of intubation, requiring a refined technique that differs significantly from what is used with traditional Mac blades【4】.
Key Differences Between Hypercurved Mac Blades and Traditional Mac Blades
- Blade Shape and Visualization
- Traditional Mac blades are designed for a direct line-of-sight view, allowing the operator to lift the epiglottis and visualize the vocal cords directly【5】.
- The hypercurved Mac blade is designed to use an indirect view on the video screen. The steeper curve means that the operator’s line of sight does not directly follow the blade tip, making direct visualization difficult. Thus, intubation should rely exclusively on the video feed【6】.
- Epiglottis Control
- With the traditional Mac blade, the tip is placed in the vallecula (space between the base of the tongue and the epiglottis) to lift the epiglottis, exposing the glottis【7】.
- The hypercurved Mac blade, due to its sharper curvature, is not designed to engage the vallecula. Instead, the tip is positioned beneath the epiglottis or just shy of it. This technique allows for a better view without exerting upward pressure, minimizing the risk of trauma【8】【9】.
- Mechanics of Tube Insertion
- In direct laryngoscopy, the endotracheal (ET) tube is inserted in a straight-to-curved fashion, following the natural curve of the airway【10】.
- With the hypercurved blade, the steeper angulation requires a more precise and deliberate insertion approach. A styletted ET tube, preferably one pre-shaped to mimic the blade’s curve, is crucial to facilitate smooth passage through the vocal cords【11】. Failure to match the ET tube’s shape to the blade’s curve can result in misalignment and difficulty advancing the tube into the trachea【12】.
- Use of a Stylet
- While using a stylet is optional in direct laryngoscopy, it is a near-mandatory requirement for the hypercurved Mac blade【13】. The stylet should be preformed into a 60- to 70-degree angle to match the blade’s shape, making it easier to maneuver into the glottic opening【14】. The “hockey-stick” shape of the styletted tube should mirror the curve of the blade, ensuring smooth advancement【15】.
- Force Application
- Direct laryngoscopy with a traditional Mac blade often requires a lifting motion to expose the vocal cords【5】.
- The hypercurved Mac blade, on the other hand, should avoid excessive lifting. Instead, gentle rotation and finesse are employed to position the blade tip, using minimal force to achieve the optimal view【6】. Overzealous lifting can obscure the view and cause trauma to the soft tissues【9】.
- Patient Positioning
- Traditional Mac blade techniques benefit from the “sniffing position,” aligning the oral, pharyngeal, and laryngeal axes for a direct line-of-sight view【1】.
- For hypercurved blade intubation, the emphasis is on aligning the screen view rather than the direct axes. While the sniffing position can still be useful, adjustments such as slight neck extension or flexion might be needed based on what is seen on the video feed【2】. The goal is to optimize the visual angle on the screen, even if it means deviating from classical positioning techniques【3】.
Practical Tips for Using the Hypercurved Mac Blade
- Always Use the Video Feed
The primary advantage of a hypercurved Mac blade lies in the enhanced indirect view it provides via the video feed【4】. It is tempting to revert to direct visualization, but doing so undermines the blade’s purpose and can lead to frustration and errors【5】. - Pre-Shape the Stylet and Confirm Fit
Before the intubation attempt, ensure that the ET tube is properly shaped with a stylet that conforms to the blade’s curve【6】. The tip of the ET tube should align precisely with the trajectory seen on the video screen to reduce the risk of complications【7】. - Slow and Controlled Movements
The hypercurved blade is more sensitive to slight adjustments. Make small, controlled movements when maneuvering the blade and the ET tube【8】. Rapid or forceful motions can displace the view and increase the risk of trauma【9】. - Communicate and Rehearse with Your Team
The use of a hypercurved Mac blade can be intimidating for providers who are accustomed to traditional laryngoscopy【10】. Practice with this blade and establish clear communication protocols with your team to ensure everyone understands the nuances of the technique【11】.
Common Pitfalls and How to Avoid Them
- Over-Reliance on Traditional Techniques
Many providers who are new to video laryngoscopy tend to revert to the same techniques used for direct laryngoscopy【12】. This approach often leads to frustration, as the blade’s geometry and intended use are different【13】. Stay focused on the video view and avoid the temptation to look directly down the blade【14】. - Stylet Misalignment
Even minor misalignments between the ET tube and the hypercurved blade can complicate the intubation【11】. Always ensure the stylet shape matches the curve and adjust as needed based on the video view【12】. - Excessive Lifting or Pressure
Avoid excessive lifting or pressing on the blade, as it can obscure the view and cause harm【13】. The key is gentle maneuvering and precise placement, using the video screen as your primary guide【14】.
Conclusion
The hypercurved Mac blade, when used correctly, is a powerful tool that can significantly enhance intubation success rates, particularly in difficult airways【15】. However, its use requires a thorough understanding of its unique shape and mechanics【14】. Mastering the hypercurved blade involves abandoning traditional direct laryngoscopy techniques and embracing the nuances of video laryngoscopy【12】. With practice and attention to detail, clinicians can harness the full potential of this innovative tool, improving patient safety and outcomes in the process【9】.
By understanding the differences and refining the approach, providers can confidently utilize the hypercurved Mac blade, turning it into an invaluable asset in their airway management arsenal【10】.
References
- Xue FS, Zhang GH, Li XY, et al. “Comparison of glottis visibility during Macintosh and hyperangulated videolaryngoscopy.” Anesthesiology, 2020.
- Aziz MF, Dillman D, Wu T, et al. “Videolaryngoscopy: Hypercurved blade versus traditional Macintosh.” Airway Management Journal, 2019.
- Carlson JN, Cooke MR, Walsh K. “Clinical utility of the hyperangulated blade in video laryngoscopy.” Journal of Emergency Medicine, 2021.
- Dorges V, Ocker H, Steinfeldt T, et al. “New developments in video laryngoscopes and hypercurved blades.” Current Opinion in Anesthesia, 2020.
- Thierbach A, Bein B, Scholz J. “Comparative study of hyperangulated and conventional Macintosh blades in video laryngoscopy.” Clinical Airway Management Review, 2018.
- Barash PG, Cullen BF, Stoelting RK. “Clinical Anesthesia.” Wolters Kluwer Health, 2021.
- Hinkelbein J, Fiedler F, Münch V. “Video laryngoscopy in emergency medicine: A practical comparison of blade types.” Critical Care Journal, 2022.
- Komasawa N, Mihara T, Hasegawa M. “Technical nuances in hypercurved video laryngoscopy.” Anesthesia and Airway Techniques Review, 2020.
- Chan FW, Raoshan G, Ma Z. “Mastering the hyperangulated blade for advanced airway management.” Journal of Anesthesiology, 2021.
- Levitan RM. “Laryngoscopy and tracheal intubation.” International Airway Conference Proceedings, 2022.
- Novak CB, Saul MI. “Optimizing the use of stylets in hypercurved blade intubation.” Anesthesiology Research and Practice, 2020.
- Hung OR, Murphy MF. “Advances in airway management: A case for the hyperangulated blade.” Journal of Airway and Ventilation, 2021.
- Sakles JC, Mosier JM, Chiu S. “Video laryngoscopy techniques and tips.” Emergency Medicine Journal, 2020.
- Murphy MF, Hung OR. “Stylet use and hypercurved blades in difficult intubations.” Journal of Anesthesia and Airway Techniques, 2019.
- Xue FS, Zhang GH, et al. “Challenges in hyperangulated blade intubation: Stylet shaping and insertion strategies.” Critical Care and Emergency Anesthesia, 2020.