There’s a number we throw around in medicine.
0.8.
We say it like it’s fixed. Predictable. Reliable.
But it isn’t.
That number… is a compromise.
And unless you understand why it exists, you will struggle to understand what’s happening when it starts to drift.
The Relationship: Ventilation vs Perfusion
At its core:
-
Ventilation (V) = air reaching the alveoli
-
Perfusion (Q) = blood reaching the alveoli
The V/Q ratio is simply:
- Air available for gas exchange ÷ Blood available to carry that gas
Under normal conditions:
-
Ventilation ≈ 4 L/min
-
Perfusion ≈ 5 L/min
So:
V/Q = 4 / 5 = 0.8 [1]
That’s where the number comes from.
Not perfection.
Just physiology doing its best under real-world constraints.
Why It’s Not 1.0
A perfect system would be:
V/Q = 1
Equal air. Equal blood. Ideal exchange.
But the lungs aren’t built that way.
Because gravity exists.
Because structure matters.
Because distribution is uneven.
Gravity Changes Everything
In an upright patient:
-
Blood is pulled downward → bases receive more perfusion
-
Ventilation also increases toward the bases… but less dramatically
So:
-
Bases: high perfusion relative to ventilation → low V/Q (~0.6)
-
Apices: low perfusion relative to ventilation → high V/Q (~3.0) [2]
Across the lung, this averages to:
0.8
Not perfect.
But functional.
The Part Most People Miss
The lung is not a single system.
It’s thousands of micro-systems.
Each alveolus has its own V/Q.
Each region is slightly mismatched.
And somehow…
It still works.
Until it doesn’t.
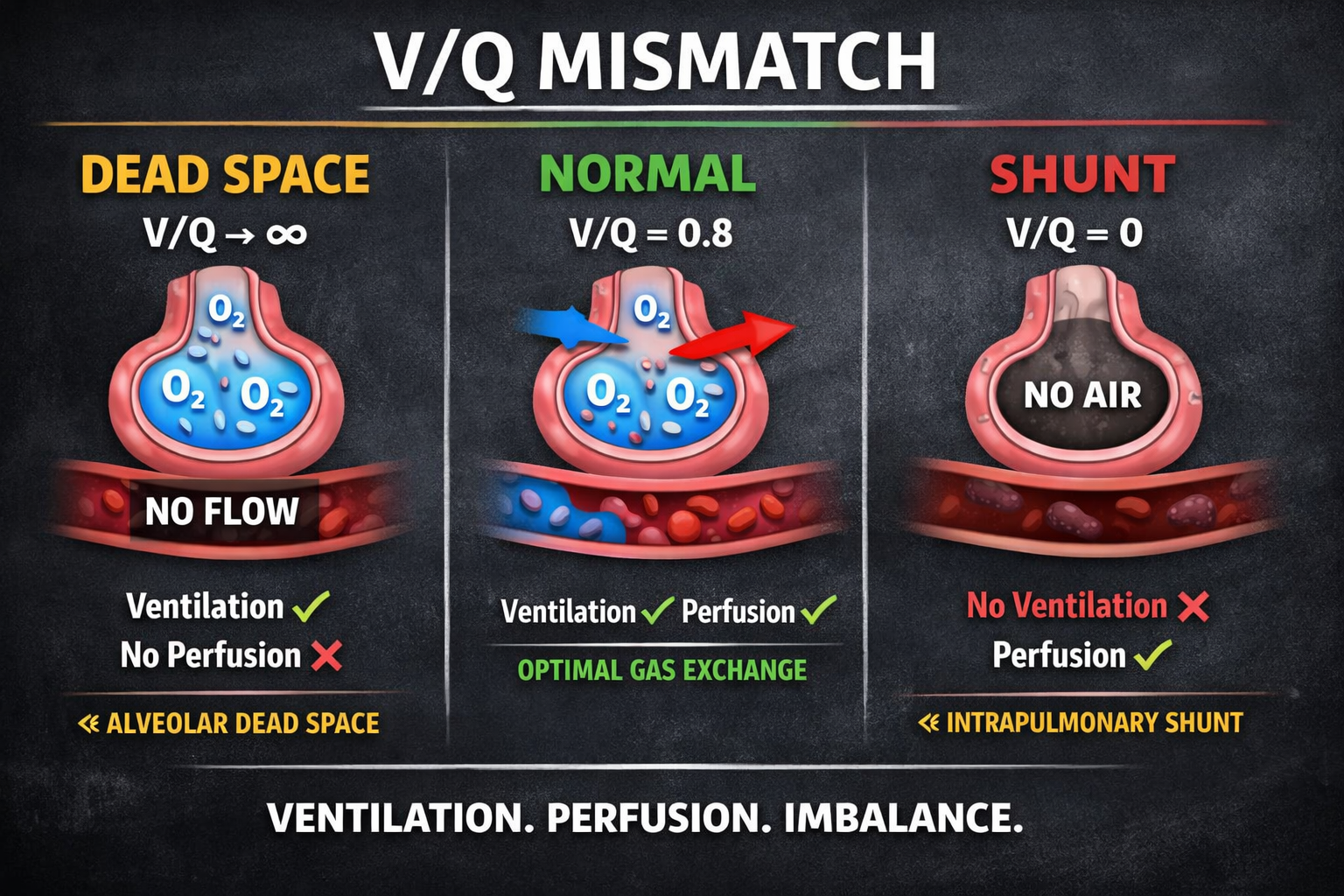
When It Breaks: Understanding V/Q Mismatch
V/Q mismatch isn’t one condition.
It’s a failure of alignment between air and blood.
And it exists on a spectrum.
But to truly understand it…
You have to understand the extremes.
The Extremes Define Everything
1. Dead Space — (V/Q → ∞)
Let’s pause here.
Because this is where people nod… but don’t actually understand.
What does (V/Q → ∞) mean?
-
V = ventilation (air)
-
Q = perfusion (blood)
So:
V/Q = Air ÷ Blood
Now imagine this:
-
Air is present
-
Blood flow is approaching zero
Mathematically:
-
If Q → 0
-
Then you are dividing by a number approaching zero
And when you divide by something approaching zero…
→ The result becomes infinitely large (∞)
Translate that into physiology
You have:
-
Air reaching the alveoli ✅
-
But no blood to receive it ❌
So:
-
Oxygen enters the lung
-
But never enters circulation
This is:
- Alveolar Dead Space
Clinical Example
-
Pulmonary embolism
-
Severe hypotension
-
Capillary collapse
In these situations:
-
Ventilation is intact
-
Perfusion is absent
So:
V/Q → ∞
The Reality
You can give 100% oxygen…
And it won’t matter.
Because there is no blood there to carry it.
2. Shunt — (V/Q → 0)
Now flip it.
-
Blood is flowing
-
Air is not
So:
-
V → 0
-
Q remains present
Result:
V/Q → 0
What does that mean?
-
Blood passes through the lungs
-
But never sees oxygen
Examples:
-
Pneumonia
-
Pulmonary edema
-
Atelectasis
-
Airway obstruction [3]
The Difference That Matters
| Condition | Ventilation | Perfusion | Result |
|---|---|---|---|
| Dead Space | Present | Absent | Wasted ventilation |
| Shunt | Absent | Present | Wasted perfusion |
The Middle Ground: Where Most Patients Live
Most patients are not at the extremes.
They exist in:
Low V/Q states (most common)
-
Ventilation reduced
-
Perfusion maintained
Examples:
-
COPD
-
Asthma
-
Pneumonia
This leads to:
→ Hypoxemia [4]
High V/Q states
-
Ventilation preserved
-
Perfusion reduced
Examples:
-
Pulmonary embolism
-
Shock states
-
Reduced cardiac output [5]
The Body Tries to Fix It
The body is not passive.
It adapts.
Hypoxic Pulmonary Vasoconstriction
-
Poorly ventilated areas → blood vessels constrict
-
Blood is redirected to better ventilated alveoli
An attempt to rebalance V/Q [6]
But this system has limits.
And when those limits are exceeded…
You see clinical deterioration.
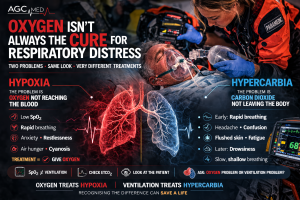
Fixing the Problem: Treat the Mechanism, Not the Number
This is where good clinicians separate themselves.
Low V/Q (Ventilation Problem)
Fix ventilation:
-
Bronchodilators
-
Positive pressure ventilation
-
PEEP and recruitment
-
Secretion clearance
Oxygen helps…
But doesn’t solve the root cause.
High V/Q (Perfusion Problem)
Fix perfusion:
-
Anticoagulation (PE)
-
Fluids / vasopressors
-
Improve cardiac output
Again…
Oxygen alone is not the answer.
The Hard Truth
You can oxygenate the alveoli perfectly…
But if blood isn’t there—
It’s meaningless.
And you can have perfect perfusion…
But if the alveoli are flooded—
It’s meaningless.
The Takeaway
That number—0.8—
Is not something to memorize.
It’s something to understand.
Because once you understand:
-
Why ventilation is ~4
-
Why perfusion is ~5
-
Why gravity distorts everything
-
Why mismatch is normal… until it isn’t
-
Why (V/Q → ∞) means no blood
-
Why (V/Q → 0) means no air
Then something changes.
You stop chasing oxygen saturations.
You stop reacting to numbers.
And you start asking the only question that matters:
- Where is the failure — air or blood?
And that’s where real medicine begins.
References
-
West JB. Respiratory Physiology: The Essentials, 11th ed.
-
Levitzky MG. Pulmonary Physiology, 9th ed.
-
Hall JE. Guyton and Hall Textbook of Medical Physiology, 14th ed.
-
West JB. Ventilation-perfusion relationships. Comprehensive Physiology. 2012.
-
Lumb AB. Nunn’s Applied Respiratory Physiology, 8th ed.
-
Sylvester JT et al. Hypoxic pulmonary vasoconstriction. Physiol Rev. 2012.