Acute Respiratory Distress Syndrome (ARDS) remains one of the most challenging and deadly respiratory conditions in critical care, characterized by profound hypoxemia, reduced lung compliance, and bilateral pulmonary infiltrates. It is not a single disease, but a syndrome, triggered by a variety of direct or indirect insults that lead to alveolar damage and non-cardiogenic pulmonary edema.
Healthcare professionals across EMS, the Emergency Department, and the ICU must recognize ARDS early, implement evidence-based strategies, and understand when to escalate care. This guide provides a unified approach to pathophysiology, diagnostics, and treatment based on current best practices, including the ARDSnet protocol and advanced therapies.
Pathophysiology of ARDS
ARDS occurs when the alveolar-capillary membrane is disrupted due to a systemic or pulmonary insult. This leads to:
- Increased permeability
- Leakage of protein-rich fluid into alveoli
- Surfactant dysfunction
- Loss of alveolar recruitment
The disease progression can be broken into three phases [1]:
- Exudative Phase (0–7 days): Marked by capillary leak, alveolar edema, and hypoxemia.
- Proliferative Phase (7–21 days): Type II pneumocyte proliferation, beginning of resolution.
- Fibrotic Phase (>21 days): Potential fibrosis, stiff lungs, prolonged ventilation.
Common Causes:
- Direct lung injury: Pneumonia, aspiration, inhalation injury, pulmonary contusion.
- Indirect injury: Sepsis, pancreatitis, major trauma, transfusion-related lung injury (TRALI) [2].
Recognizing ARDS
Clinical Features
- Acute onset of dyspnea
- Refractory hypoxemia despite high FiO₂
- Tachypnea, respiratory distress, crackles
- Often requires escalating oxygen support
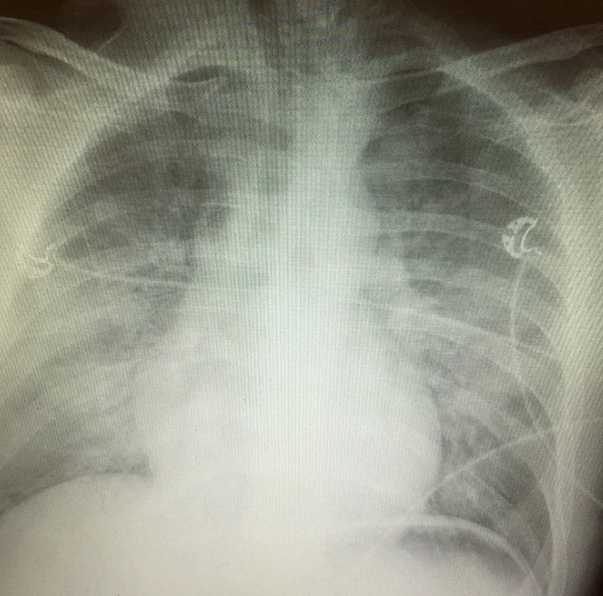
Radiographic Clue
- Ground-glass opacities or
- bilateral infiltrates on CXR or CT,
- without features of cardiac failure [3].
The P:F Ratio: Understanding Oxygenation Impairment
A central feature in diagnosing and grading ARDS is the PaO₂/FiO₂ (P:F) ratio:
- PaO₂: Measured from an arterial blood gas (ABG)
- FiO₂: Fraction of inspired oxygen (room air = 0.21 or 21%)
Example: If PaO₂ = 70 mmHg and FiO₂ = 0.7 → P:F = 100 → Severe ARDS
ARDS Severity by P:F Ratio [4]:
- Normal: >400
- Mild ARDS: 200–300
- Moderate ARDS: 100–200
- Severe ARDS: <100
Always assess the P:F ratio with the patient on PEEP ≥5 cm H₂O to ensure accuracy in classification.
Management of ARDS
- Treat the Underlying Cause
Management begins with identifying and treating the inciting pathology:
- Sepsis → Early antibiotics
- Aspiration → Suctioning, antibiotics if infected
- Trauma or pancreatitis → Source control
- TRALI → Discontinue transfusions immediately [2]
- Lung-Protective Ventilation (ARDSnet Protocol)
ARDSnet provides the gold standard for safe mechanical ventilation [5]:
Goals:
- SpO₂: 88–95%
- PaO₂: 55–80 mmHg
- Tidal Volume: 4–6 mL/kg Ideal Body Weight
- Plateau Pressure: <30 cm H₂O
- PEEP/FiO₂ Adjustments: Based on severity and P:F ratio
- Wait 5–10 minutes between FiO₂ or PEEP changes to assess effect [5]
- Adjunct Therapies
Prone Positioning
- Improves oxygenation in moderate-to-severe ARDS (P:F <150)
- Should be started within 36 hours of intubation
- Performed for 12–16 hours per session
- Shown to reduce mortality [6]
Neuromuscular Blockade
- May improve oxygenation and ventilator synchrony in early, severe ARDS
- Recommended only for the shortest duration necessary [7]
Fluid Strategy
- Once hemodynamically stable, switch to conservative fluid management to reduce pulmonary edema and improve lung function [8]
Inhaled Vasodilators
- e.g., Inhaled nitric oxide or epoprostenol
- May transiently improve oxygenation but no proven mortality benefit
- Rescue Therapy: ECMO
In cases of refractory hypoxemia despite optimized care:
- Veno-venous ECMO provides gas exchange while minimizing ventilator-induced lung injury
- Consider ECMO if:
- P:F ratio <80 for >6 hours or <50 for >3 hours
- High plateau pressures with respiratory acidosis [9]
Transport and Prehospital Considerations
Even before the ICU, steps should be taken to preserve oxygenation and prevent iatrogenic harm:
- Use PEEP valves if bagging intubated patients
- Monitor for hypoxia and barotrauma
- Maintain SpO₂ 88–95% rather than chasing 100%
- Communicate ventilation strategy during handover to ensure ARDSnet protocols are continued
Conclusion
ARDS is not just a respiratory failure—it’s a syndrome of systemic inflammation and alveolar injury that requires precision, coordination, and vigilance from every provider across the continuum of care.
By understanding the P:F ratio, utilizing the ARDSnet protocol, and leveraging adjunct therapies like proning, NMBA, and ECMO when necessary, we can improve oxygenation, avoid ventilator-induced damage, and improve survival rates.
Every patient deserves safe, evidence-based, and compassionate respiratory care—from the street to the ICU and beyond.
References
- Matthay MA, Ware LB, Zimmerman GA. (2012). The acute respiratory distress syndrome. J Clin Invest. 122(8):2731–2740.
- Bellani G, et al. (2016). Epidemiology, Patterns of Care, and Mortality in ARDS. JAMA. 315(8):788–800.
- Desai, S.R. (2003). Ground-glass opacification in ARDS. Radiology. 228(3):725–734.
- Ranieri VM, et al. (2012). The Berlin Definition of ARDS. JAMA. 307(23):2526–2533.
- ARDSnet. (2000). Ventilation with lower tidal volumes as compared with traditional tidal volumes. N Engl J Med. 342(18):1301–1308.
- Guérin C, et al. (2013). Prone positioning in severe ARDS. N Engl J Med. 368:2159–2168.
- Papazian L, et al. (2010). Neuromuscular blockers in early ARDS. N Engl J Med. 363:1107–1116.
- Wiedemann HP, et al. (2006). Fluid management strategy in ARDS. N Engl J Med. 354(24):2564–2575.
- Combes A, et al. (2018). ECMO for severe ARDS. N Engl J Med. 378(21):1965–1975.



Hey There. I found your blog using msn. That is a very
smartly written article. I’ll be sure to bookmark it
and return to read more of your helpful information. Thanks for the
post. I will definitely comeback.
Also visit my page: burn peak weight loss reviews